Bitspec
The Admissions architecture itself influences demographic outcomes in medical schools- Ontario, Canada
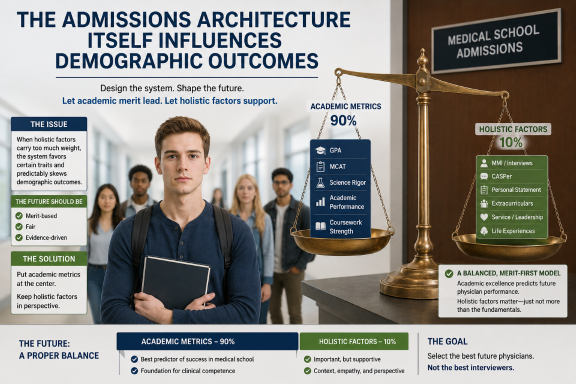
Fig. 1 Admission Architecture Medical Schools
For many years, public discussions about medical school admissions focused almost entirely on one question:
“Who is the most qualified candidate?”
But modern admissions systems reveal a deeper reality:
The way a system defines merit directly shapes who succeeds within it.
Admissions systems are not passive.
They are engineered structures built around institutional priorities, policy decisions, and philosophical assumptions about what society believes a future physician should look like.
As those assumptions change, demographic outcomes change with them.
Admissions systems are designed systems
Medical school admissions are often presented as neutral and objective. In reality, every admissions framework embeds value judgments.
A system that heavily weights:
- GPA,
- advanced science performance,
- standardized academic testing,
will produce one demographic and cognitive profile.
A system that heavily weights:
- interpersonal communication,
- behavioural interviews,
- situational judgment testing,
- autobiographical narratives,
- and perceived empathy,
will produce another.
Neither system is accidental.
The architecture itself determines which traits are rewarded.
The Canadian shift toward holistic admissions
Over the past several decades, many medical schools in Canada have moved away from admissions models centered primarily on academic metrics.
Institutions increasingly adopted:
- MMIs (Multiple Mini Interviews),
- CASPer situational judgment testing,
- autobiographical sketches,
- contextual admissions policies,
- and broad “holistic review” frameworks.
The stated goal was clear:
to produce physicians who were not only scientifically capable, but also:
- communicative,
- collaborative,
- emotionally aware,
- socially accountable,
- and patient-centered.
These changes reflected broader institutional beliefs about modern healthcare.
Demographic outcomes changed
As admissions architectures changed, the demographic composition of medical schools changed as well.
Women became the majority in many medical programs across Canada and several other Western countries.
This raises an important institutional question:
Did demographics change because applicant ability changed, or because the system changed what it rewarded?
The answer is likely both.
Research examining tools such as CASPer and MMIs has reported average group differences in certain behavioural and communication-oriented domains. Studies have also raised concerns about socioeconomic effects, coaching advantages, and the role of professional communication style in scoring outcomes.
This does not automatically prove intentional discrimination.
However, it does demonstrate something structurally important:
Selection systems influence demographic outcomes because selection criteria are not socially neutral.
The redefinition of merit
One of the most controversial aspects of modern admissions is that merit itself has been redefined.
Historically, medicine emphasized:
- academic rigor,
- scientific achievement,
- memorization,
- analytical reasoning,
- and technical capability.
Modern systems increasingly incorporate:
- empathy signaling,
- communication style,
- ethical framing,
- behavioural performance,
- and interpersonal evaluation.
Supporters argue this produces physicians better suited to contemporary healthcare systems.
Critics argue that the weighting may now disproportionately favor certain behavioural profiles while underweighting:
- analytical intensity,
- technical orientation,
- or cognitively diverse personality types.
This is not merely a demographic discussion.
It is a philosophical debate about: what society believes medicine should optimize for.
Equity versus outcome equality
Another tension emerges around the meaning of “equity.”
Some institutions define equity as:
- equal opportunity under common rules.
Others define equity as:
- achieving broader representation across groups.
Others define it as:
- selecting competencies believed to improve patient care regardless of demographic outcome.
These approaches can produce very different admissions structures.
A system may apply identical rules to all applicants while still producing unequal demographic outcomes if the rewarded traits correlate differently across populations.
This is why admissions architecture matters so profoundly.
Every selection system creates trade-offs
No admissions system is neutral.
If a school emphasizes:
- MCAT science scores,
- GPA,
- and advanced quantitative reasoning,
it may select more heavily for analytical academic performance.
If it emphasizes:
- MMIs,
- CASPer,
- and interpersonal evaluation,
it may select more heavily for behavioural and communication performance.
Every weighting decision changes:
- who applies,
- who succeeds,
- who self-selects out,
- and ultimately what the profession becomes.
The profession itself is shaped by the architecture of entry.
The larger policy question
The deeper question is not whether communication matters.
Almost everyone agrees that it does.
The deeper question is: how much should different competencies be weighted relative to one another?
Medicine requires simultaneously:
- scientific reasoning,
- technical competence,
- diagnostic accuracy,
- emotional regulation,
- communication,
- ethical judgment,
- and teamwork.
No system can maximize every trait equally.
Admissions architecture therefore, becomes a policy instrument that reflects institutional priorities about what kinds of physicians should dominate the future healthcare system.
Conclusion
The modern debate over medical school admissions is not simply about fairness between applicants.
It is about institutional design.
When admissions systems change:
- demographic outcomes change,
- professional culture changes,
- workforce composition changes,
- and eventually healthcare systems themselves evolve.
The architecture of selection determines the architecture of the profession.
And once institutions understand that reality, admissions criteria are no longer just technical procedures.
They become social policy.
An article blog written with ChatGPT version. 5.5 support May 14, 2026
When you subscribe to the blog, we will send you an e-mail when there are new updates on the site so you wouldn't miss them.