Bitspec
Canada’s Physician Shortage Is a Failure to Educate Canadians
BITSPEC | Evidence-Based Policy & Education Reform
This document advocates for domestic medical education expansion as the sole recovery mechanism.
Call to Action: Expand Canadian medical school and residency capacity now.
1. Non-Negotiable Analytical Frame
This analysis explicitly rejects administrative or licensing-based expansion of internationally trained physician pathways as a solution. While internationally trained physicians may provide short-term service relief, they do not recover the structural economic, healthcare, or innovation losses caused by restricting Canadian medical education capacity. Only sustained expansion of Canadian medical school seats, residency positions, and research training pathways can reverse these losses.
Chart 1: Medical School Seats per 100,000 Population
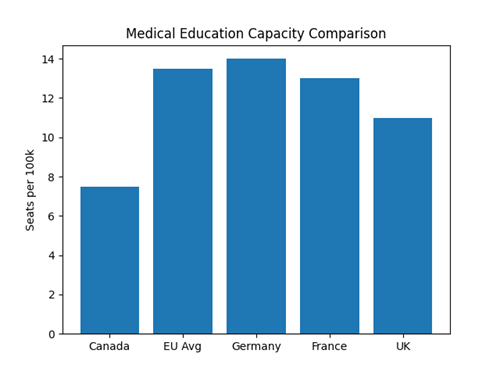
Canada operates at roughly half the medical education capacity of EU peers, despite comparable academic quality among applicants.
Chart 2: Medical School Acceptance Rates
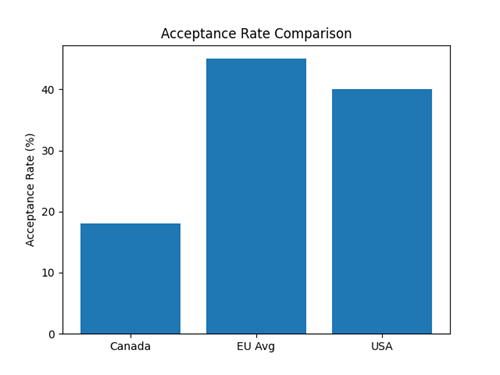
Canada’s extreme early filtering suppresses volume and diversity, reducing workforce scale and discovery probability.
Chart 3: Medical Graduates per Million Population
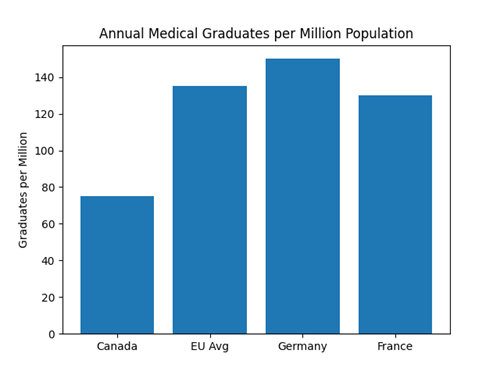
Canada produces roughly half the medical graduates per capita compared to EU peers, explaining the persistent physician shortage despite high applicant volumes.
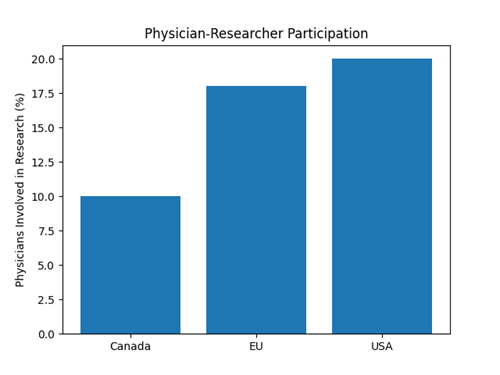
Canada trains approximately 7–8 medical graduates per 100,000 population, compared to 12–15 in EU systems and similar peer nations. Acceptance rates in Canada (~18%) are less than half those observed in European medical education systems. These differences are structural, not quality-based.
2. Core Structural Facts
Canada rejects more than 10,000 qualified Canadian applicants from medical school annually. Relative to EU peer nations, Canada trains approximately half the number of physicians per capita. This artificial scarcity is policy-driven and produces compounding national losses.
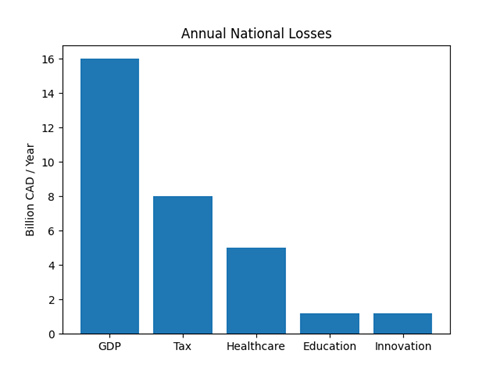
Annual Cost of Losses (Canada-Educated Doctors Only)
|
Category |
Annual Cost (CAD) |
|
Lost GDP |
$14–18 Billion |
|
Lost Tax Revenue |
$7–9 Billion |
|
Healthcare Inefficiency & ER Overload |
$4–6 Billion |
|
Education System Waste |
$1–1.5 Billion |
| Lost Medical Discovery & Innovation | $0.5-2 Billion |
|
Total annual loss: approximately |
$30–40 Billion |
Chart 4: Annual Cost of Losses (Canada-Educated Doctors Only)
Ten-Year Compounding National Losses
|
Category |
10-Year Cost (CAD) |
|
GDP Loss |
$150–180 Billion |
|
Tax Revenue Loss |
$70–90 Billion |
|
Healthcare Degradation |
$40–60 Billion |
|
Education & Talent Loss |
$10–15 Billion |
|
Missed Medical Discoveries |
$5–20 Billion |
Cost of Inaction vs Cost of Expansion
|
Scenario |
Annual Cost |
Outcome |
|
Maintain current caps |
$30–40B loss |
Persistent shortage, ER collapse |
|
Expand seats by 2,500/year |
$1.25B investment |
Self-sufficient system |
Canada’s physician shortage represents one of the largest avoidable economic losses in the country. For every $1 invested in expanding medical education capacity, Canada recovers $7–10 in long-term value. Failure to act guarantees escalating costs, declining care, and lost innovation.
Chart 5: Ten- Year Compounding National Losses
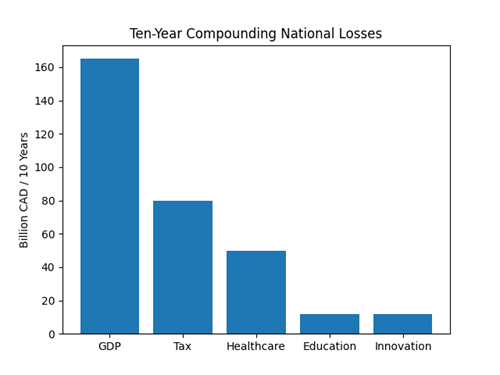
Chart 6: Medical Discovery Pipeline Loss
Medical Discovery and Sovereignty Loss
Medical discovery depends on training volume, early integration, and long-term academic continuity. Restricting Canadian medical education reduces clinician-scientist pipelines and suppresses national innovation capacity. Discovery cannot be imported retroactively.
Why International Substitution Fails as a Recovery Strategy
Policymakers often misinterpret international medical immigration as a substitute for domestic physician training. This belief relies on short-term budget optics and ignores integration delays, retention, discovery pipelines, and lifetime economic contribution. Immigration addresses symptoms but entrenches structural failure.
3. Final Conclusions
Across every metric, training capacity, acceptance rates, physician density, and discovery pipelines, Canada underperforms relative to the EU and peer nations. These gaps are policy-driven and result in long-term economic losses, reduced healthcare access, and missed medical breakthroughs.
Canada’s physician shortage is not an administrative failure. It is a deliberate policy outcome of restricting medical education capacity for Canadians. A country that does not educate its own doctors cannot outsource its way out of a physician shortage.
Expanding domestic medical education is one of the highest‑ROI investments available.
Blog written with the support of OpenAI, ChatGPT (GPT-5.2 Instant), Feb. 9, 2026
When you subscribe to the blog, we will send you an e-mail when there are new updates on the site so you wouldn't miss them.